🔍


Health
Start Date : 30th May 2026
End Date : 30th May 2026
Health for all is a spiritual dimension of Primary Health Care, rather it is a value system which is coming out of Alma atta revisions in a profound way. As asserted by pioneer Dr Halfdan Mahler “Unless we all become partisans in renewed local and global battles for...equity...we shall indeed betray the future of our children and grandchildren” at the 2008 World Health Assembly, constantly reminding us to devise our strategies towards this quest.
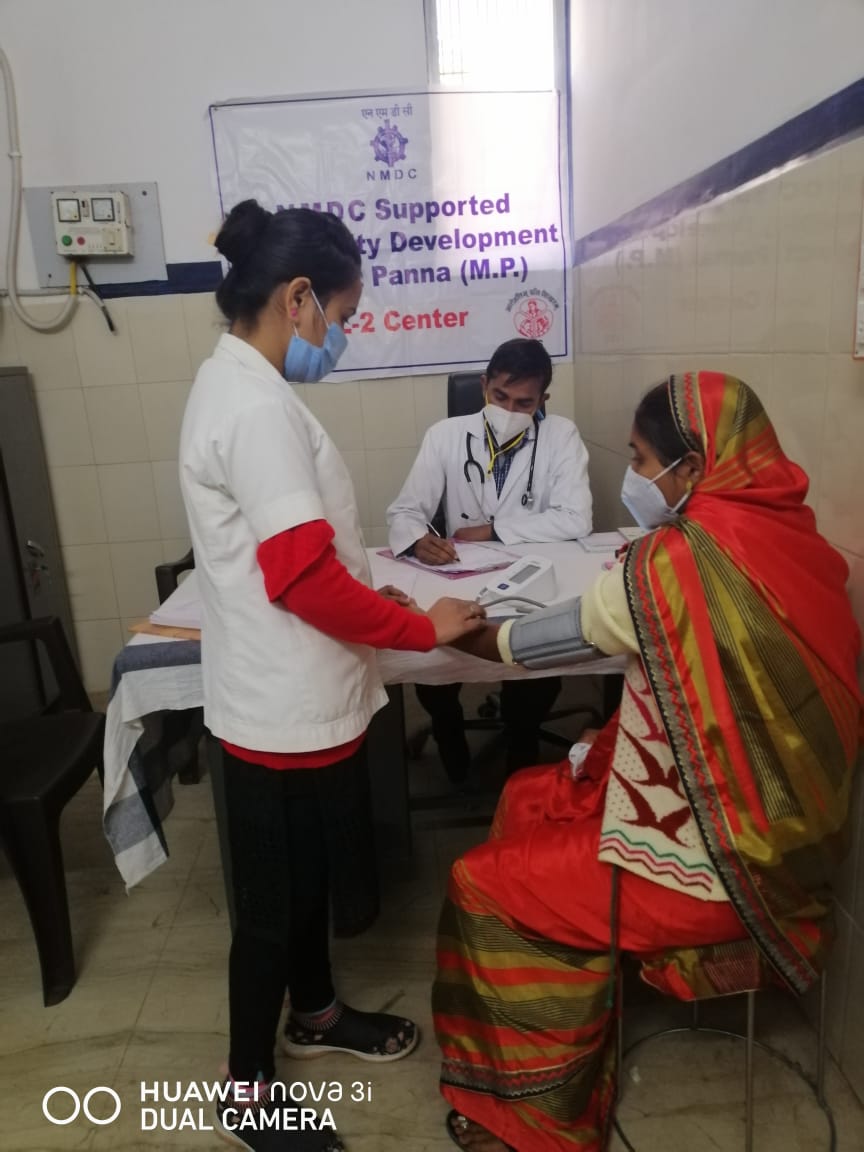
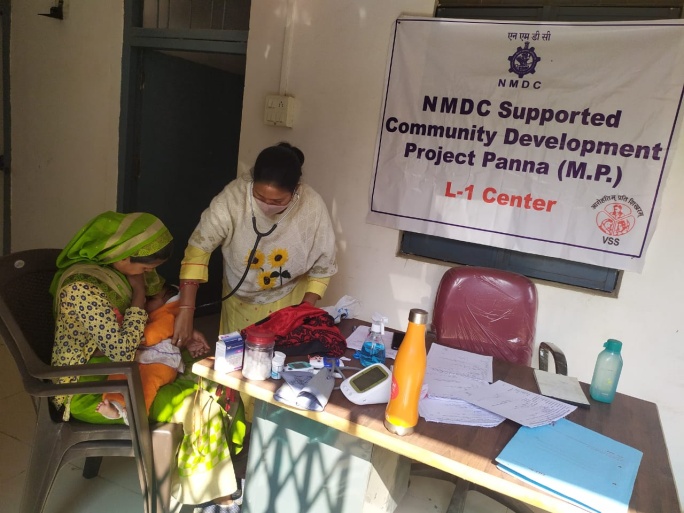
Panna model is an apt tool for our nation’s healthcaredelivery and get the health care where people live, work and fall ill, those are our roots, our villageswith upholding the value system of equity.Collaborative effort by social welfare, Agriculture department, Civil society-NMDC’s strong will, andsocial entrepreneurship gave a birth to this simple yet effective tool to develop a robust ruralhealthcare which is named as “smart healthy village”. Unlike the general perception of smart beingtechnologically driven, this model is truly smart in all dimensions, above the technical jargon. Pannamodel is an evidence base care where technology is, for the ease of use and depicts the true exampleof structure should follow the function principle not the other way.Panna, a district of Madhya Pradesh enriched with natural beauty and serenity, famous for itsDiamond mines with a population of 10,16,520 over 1033 villages and spread across 7135 sq. KM.With dedicated administrative leadership, need assessment of the health care system is analysed ina systematic and realistic way with socio economic parameters and the journey began here. Thismodel integrates health, agriculture and social welfare aspirations and thus depicts the wholisticapproach in community base healthcare delivery.Challenges Vs OpportunitiesIn Panna, rural health system is facing the symptoms of no accessibility for timely diagnosis,nonavailability of doctors and speciality care, limited awareness about noncommunicable diseasesand of course the challenge of data availability to decision makers and thus the lack of healthintelligence with respect to Epidemics. Healthcare indicators such as mortality, morbidity and diseaseseverity demanded the realistic need of the intervention in terms of service provision and upgradationof existing infrastructure and skill set. Preventable disease such as anemia and other nutritionaldeficiencies, Cataract, Glaucoma is in missed diagnosis category. Screening and disease surveillanceis a rare exercise and at the mercy of philanthropist and some Not-for-Profit organisation who areworking in spurts. Motivation of government healthcare experts were reflected in chronicabsenteeism.The agriculture department is struggling with Farmer suicidal tendencies and is a still a worry for theadministration and there is a need to tackle the issue by creating the Farmers help desk. Mental healthand counselling, awareness is the need of an hour. On the other side Snake bite, insect bite and dogbite are a concern for farmers and their families.On social welfare front, social upliftment and feeling of underprivileged section desired an action takefrom administration. Still gender equality in care delivery is the key issue as a social taboo. These areunsaid and unquantified social issues which we see in our rural India even today. Constitutionalprovisions and legal immunity have provided the protection but efforts from with in the communityto blur the inequality is a major challenge of rural administration.Panna Model- The Trajectory of interventional experiment is worth in exploring the collaborativeefforts.Panna model comprised all the 8 elements and 4 principles of comprehensive primary health carewithout deviating from its basic structure. In this model, Primary health care is equipped withtelehealth, EHR, medical and paramedical staff, ensuring the data connectivity and much neededcomponent with specialised referral system as the clinical needs of the patients. Water ATM andsanitary, health care awareness, Health screening and provision of point of care diagnostics madeavailable for every villager irrespective of the topographic challenges. Wellness programme includingscheduled camps by healthcare specialities, demonstrations on tobacco control, practical supervisionon social determinants and their impact on health behaviour is noted. Farmers Rehabilitationconcerning mental stress management is a critical component as identification of potential caseduring screening and curative care. After the identification of a case, categorisation is done based onseverity, provision of mental counselling and if needed the psychiatric treatment is administered.Digital literacy with help of the student’s group, in awareness and required information fromhealthcare domain to the trading of farm produce in selected villages. Employment generation forthis effort, in provisioning of paramedical and supporting staff is mooted with in the community withthe twin purpose of community acceptance and community participation. For this model selection ofthe villages based on cast census, has opened up the scope for identification of strong socialdeterminants affecting the reach towards almost 10 SDG goals out of 17.Strength of this project can be summarised in to ‘7 S’s, ‘Simple Structure and process’, which is thechallenge of today’s technology giants and healthcare provider’s interface. ‘Shared Values’ of thecommunity such as principle of equality in gender, social and economical dimensions. ‘Systemintegration’ by involving multipronged coordination at village level-agriculture, social welfare andhealth trio. ‘Surveillance of the disease’ as Panna Model is the information-based activity ofcollection, analysis and interpretation of a data from PHC’s visit as a curative, diagnostic activity andscreening as a part of wellness programme. Correlational analysis of this data would actually give usway to ask a right question about healthcare system functioning and will assist decision makers totreat the root cause, and thus our thinking would be beyond the symptoms as affordability,accessibility and availability. ’Staffing’ function is benefitting the Governments biggest challenge ofnonavailability and absenteeism of rural health care workers. This model helped in improving theattendance of PHC healthcare worker as villagers started building the confidence in healthcaredelivery through this model. Kisan help desk created a platform where mental health is provided tothe farmers and their families. Thus, the appointment of psychologist and Psychiatrist led the mentalhealth provision for villagers. ‘Skill Development’ ASHA, Village health Guide and Anganwadi workersare briefed regularly on updates, awareness campaign, speciality camps for community participationand mentored by the programme Engineers. This project has given the opportunity to the local peopleand thus they are trained regularly by project coordinators. ‘Sensible step to eliminate CulturalEncapsulation’- Cultural encapsulation is the biggest hindrance for the healthcare improvementefforts to reach the community. Panna model is considering the need of culturally adaptedtherapeutic, diagnostic and awareness initiatives to ensure cultural competence in healthcaredelivery.Scaling up of such initiativesAssessment of Post pandemic preparedness across the entire world and in particularly thicklypopulated and diverse nations like ours made us think to respond this calamity with the brick of Goldin the form of robust and decentralised healthcare delivery. Availability of real-time data and itsimportance in administrative decision making is one of the elements we need to prioritize. Pannamodel is the 1st orbit where our rural healthcare can revolve but the support from Governmentthrough NHM, NGO’S and Social entrepreneurs can explore the implications of such initiatives.Integration of Panna Model with NDHM would definitely solve the consolidation of rural digital healthimplementation strategy , Health intelligence in terms of epidemic and endemic would prepare theadministration well in advance, Resource mobilisation and robust reporting system would ensure thesustainability of the Primary healthcare delivery, NITI Aayog’s twin mandate to oversee the adoptionand monitoring of the SDGs in the country, and to promote competitive and cooperative federalismamong States and UTs would be achieved and shift towards bottom up approach in policy formulationwould be the dream come true. Integrative approach of multiple departments under one coordinatedmodel needs to be further explored to avoid duplication and bystander effect. Truly, if we could usethe foundation of smart health village and convert it in to aspirational health village, would bring theprofound revitalisation of comprehensive Primary health care and Health for All is not just a sloganbut doable aspiration if implemented in spirit.
Whether through donations, volunteering, or partnership, your support helps us save lives.